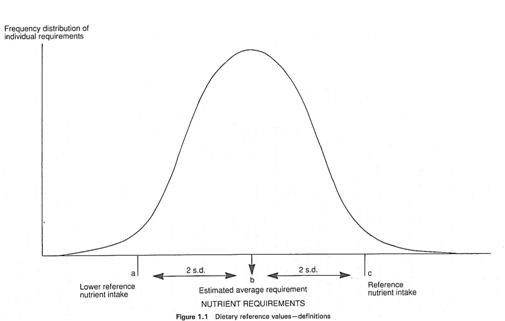
Meaningful estimates of nutrient requirements must consider the distribution of requirements within a population or group. To achieve this, the COMA panel used four Dietary Reference Values (DRVs) below (also see figure 1 above).
The COMA panel set EARs for energy and estimates of the desirable intake levels (Dietary Reference Values) for dietary fibre and for fat, carbohydrate and subclasses of these. EARs and RNIs were set for protein, whilst LRNIs, EARs and RNIs were set for nine vitamins and 11 minerals. Safe intakes were set for a further four vitamins (pantothenic acid, biotin, vitamin E and vitamin K) and four minerals (manganese, molybdenum, chromium and fluoride).
Estimated Average Requirements for Energy
In 2011, SACN published its review of the available evidence on calculating basal metabolic rate (BMR) and physical activity levels (PAL), which are used to estimate energy requirements. The Henry equation was used to estimate BMR and PAL levels were revised to better reflect current physical activity levels. The calculations were based on the energy required to maintain a BMI of 22.5kg/m2, reflecting the need to encourage a shift in the population towards a healthier weight. These changes resulted in changes to estimated energy requirements within the population with values for adults increasing from previous estimates made by COMA.
This does not represent an actual change in people’s energy requirements, but a more accurate estimate of how much energy is needed for different population groups. As such, recommendations for energy consumption for the general population have not been changed and the guideline daily amounts of 2000kcal for women and 2500kcal for men continue to be used for labelling purposes.
The EARs for energy are shown in the table below.
Table 1: Estimated Average Requirements for Energy from SACN for Infants and Children (2011)
|
EARs for Infants and Children
|
|
Age
|
Males
|
Females
|
Age
|
Males
|
Females
|
|
MJ/day
|
kcal/day
|
MJ/day
|
kcal/day
|
MJ/day
|
kcal/day
|
MJ/day
|
kcal/day
|
|
INFANTS
|
CHILDREN
|
|
Breastfed
|
4 years
|
5.8
|
1386
|
5.4
|
1291
|
|
1-2 months
|
2.2
|
526
|
2.0
|
478
|
5 years
|
6.2
|
1482
|
5.7
|
1362
|
|
3-4 months
|
2.4
|
574
|
2.2
|
526
|
6 years
|
6.6
|
1577
|
6.2
|
1482
|
|
5-6 months
|
2.5
|
598
|
2.3
|
550
|
7 years
|
6.9
|
1649
|
6.4
|
1530
|
|
7-12 months
|
2.9
|
694
|
2.7
|
646
|
8 years
|
7.3
|
1745
|
6.8
|
1625
|
|
Breastmilk substitute-fed
|
9 years
|
7.7
|
1840
|
7.2
|
1721
|
|
1-2 months
|
2.5
|
598
|
2.3
|
550
|
10 years
|
8.5
|
2032
|
8.1
|
1936
|
|
3-4 months
|
2.6
|
622
|
2.5
|
598
|
11 years
|
8.9
|
2127
|
8.5
|
2032
|
|
5-6 months
|
2.7
|
646
|
2.6
|
622
|
12 years
|
9.4
|
2247
|
8.8
|
2103
|
|
7-12 months
|
3.1
|
742
|
2.8
|
670
|
13 years
|
10.1
|
2414
|
9.3
|
2223
|
|
Mixed feeding or unknown
|
14 years
|
11.0
|
2629
|
9.8
|
2342
|
|
1-2 months
|
2.4
|
574
|
2.1
|
502
|
15 years
|
11.8
|
2820
|
10.0
|
2390
|
|
3-4 months
|
2.5
|
598
|
2.3
|
550
|
16 years
|
12.4
|
2964
|
10.1
|
2414
|
|
5-6 months
|
2.6
|
622
|
2.4
|
574
|
17 years
|
12.9
|
3083
|
10.3
|
2462
|
|
7-12 months
|
3.0
|
718
|
2.7
|
646
|
18 years
|
13.2
|
3155
|
10.3
|
2462
|
|
1 year
|
3.2
|
765
|
3.0
|
717
|
|
|
|
|
|
|
2 years
|
4.2
|
1004
|
3.9
|
932
|
|
|
|
|
|
|
3 years
|
4.9
|
1171
|
4.5
|
1076
|
|
|
|
|
|
Table 2: Estimated Average Requirements for Energy from SACN for adults (2011)
|
EARs for Adults
|
|
|
Age
|
Males
|
Females
|
|
|
MJ/day
|
kcal/day
|
MJ/day
|
kcal/day
|
|
19-24 years
|
11.6
|
2772
|
9.1
|
2175
|
|
25-34 years
|
11.5
|
2749
|
9.1
|
2175
|
|
35-44 years
|
11.0
|
2629
|
8.8
|
2103
|
|
45-54 years
|
10.8
|
2581
|
8.8
|
2103
|
|
55-64 years
|
10.8
|
2581
|
8.7
|
2079
|
|
65-74 years
|
9.8
|
2342
|
7.7
|
1912
|
|
75+ years
|
9.6
|
2294
|
8.7
|
1840
|
The EAR for women who become pregnant increases by 0.8 MJ/day (200 kcal/day) but only in the final three months of pregnancy. Although energy is needed for the growth of the fetus and to enable fat to be deposited in the mother’s body, pregnant women can compensate for these extra demands by becoming less active and using energy more efficiently.
Breastfeeding mothers have increased requirements for energy, but this will depend on the amount of milk produced, the fat stores that have accumulated during pregnancy and the duration of breastfeeding.
The EARs for energy are based on the present lifestyles and activity levels of the UK population. Although an increase in energy expenditure may well have desirable health benefits for many people, the EARs given are based on current activity levels, which are relatively low. There are also EARs available for higher (such as those in active occupations) and lower (such as those who are housebound) levels.
Energy requirements are related to age, gender, body size and level of activity. Energy requirements tend to increase up to 15-18 years old. On average, boys have slightly higher requirements than girls, which persists throughout adulthood. After about 18 years, energy requirements tend to be lower, but this depends on the individual’s level of activity. By the age of 50 years, energy requirements are lower, partly due to a reduction in the basal metabolic rate (BMR) and a reduced level of activity.
The EARs for adults are based on the current lifestyle in the UK which is sedentary. The EARs were calculated by multiplying BMR by a factor – the Physical Activity Level or PAL – which reflects current levels of physical activity.
Energy EAR = BMR x Physical Activity Level (PAL)
A factor, or multiple of BMR, of 1.4-6 reflects the lifestyle of most adults in the UK. This factor is suitable for people who do little physical activity at work or in their leisure time. If people are more active, larger factors (PALs) are used. For example, a PAL of 1.9 would be appropriate for very active adults.
Dietary Reference Values for carbohydrates and fats
Table 3: DRVs (population averages) for adults for carbohydrate and fat as a percentage of energy intake
|
|
Dietary Reference Value, % of daily food energy intake (excluding alcohol)
|
Average British adult intakes, % food energy intake (Source: NDNS, 2020)
|
|
|
|
Men
|
Women
|
|
Total carbohydrate
|
50
|
47.0
|
46.6
|
|
of which free sugars
|
5
|
10.4
|
10.3
|
|
Total fat
|
35
|
35.2
|
35.7
|
|
of which saturated fatty acids
|
11
|
12.7
|
12.9
|
|
polyunsaturated fatty acids*
|
6.5
|
6.2
|
6.4
|
|
trans fatty acids
|
2
|
0.5
|
0.5
|
|
monounsaturated fatty acids
|
13
|
13.1
|
13.2
|
*An individual maximum of 10% applies (with an individual minimum of 0.2% from linolenic acid, and 1% linoleic acid). Alcohol should provide no more than 5% of energy in the diet.
Sources: Department of Health (1991) Dietary Reference Values for Food Energy and Nutrients in the United Kingdom. HMSO, London. Public Health England (2020) National Diet and Nutrition Survey Rolling Programme Years 9 to 11 (2016/2017 to 2018/2019). London, HMSO.
How should DRVs be used?
For practical purposes, the RNI should be used when assessing the dietary intake of a group.
The nearer the average intake of the group is to the RNI, the less likely it is that any individual will have an inadequate intake.
The nearer the average is to the LRNI, the greater the probability that some individuals are not achieving adequate intakes. For example, if 20% of a group is typically consuming less than the LRNI, it is likely that most of these have an inadequate intake. When planning a diet for a group the aim should be to provide the RNI.
UK Dietary Reference Values
Fat, protein, carbohydrates and alcohol provide energy. Evidence suggests that the energy mix of the diet can influence the risk of developing various diseases. Examples include consuming too much fat and coronary heart disease risk, as well as too much alcohol influencing the risk of certain cancers.
The COMA panel reviewed the evidence around the energy mix of the diet and the risk of disease. The Panel concluded that it would be useful to set DRVs for total fat (fatty acids and glycerol), fatty acid subclasses (such as saturates), sugars and starches (see Table 3).
The average intake of fibre should be;
- 30 g/day for teenagers and adults over 16 years
- 25 g/day for children aged 11-16 years
- 20 g/day for children aged 5-11 years
- 15 g/day for children aged 2-5 years
Guidelines also exist for alcohol intake. Alcohol should provide no more than 5% of energy in the diet. As some people do not drink, there are DRVs for diets containing alcohol (total energy) and not containing alcohol (food energy).
Surveys such as the National Diet and Nutrition Survey series compare current intakes of nutrients with the various DRV values to assess where problems exist and to assist in forming government policy.
How do nutrient needs vary across life stages?
Nutrient requirements alter during a lifetime. The COMA panel reviewed the evidence on which the current estimates of nutrient requirements are based. The major changes in the estimated nutrient requirements at different life stages are summarised here:
The first 4-6 months of life is a period of rapid growth and development. Breast milk (or infant formula) contains all the nutrients required during this period. Health professionals should encourage mothers to breastfeed and not give solid foods to infants before the age of 4 months.
Government advice recommends exclusive breastfeeding until 6 months of age. During the first months of life, babies can draw upon iron stores they have accumulated before birth. These iron stores are rapidly depleted, and it is important that the diet given during weaning contains enough iron to meet the baby’s needs for growth and development. Requirements for protein, thiamin, niacin, vitamin B6, vitamin B12, magnesium, zinc, sodium, and chloride also increase between 6 and 12 months. The government recommends vitamin D supplements for some infants under 1 year.
1-3 years
Energy requirements increase because children are active and growing rapidly. Protein requirements do not increase much. Young children have an increased need for all the vitamins, except vitamin D (some of which the body can now make from sun exposure on the skin). Young children need lower amounts of calcium, phosphorus, and iron but more of all the other minerals except for zinc. Parents and carers should give daily vitamin drops containing 10 micrograms of vitamin D to this age group.
In the second year of life, children continue to need energy-dense diets. Parents and carers should give young children whole milk, not skimmed or semi-skimmed. Parents and carers should also take care of the amount of dietary fibre their child eats. A diet that is too bulky due to too many high-fibre foods could lead to the child being unable to meet its energy needs by eating enough food. Parents and carers can give semi-skimmed milk after the age of 2 years if the child is getting enough energy in the diet. Parents and carers should not give skimmed milk before the age of 5 years.
4-6 years
Energy requirements continue to increase. There is a greater need for protein, all the vitamins (except C and D) and all the minerals (except iron). The RNI figure for vitamin C remains the same as for younger children. Vitamin D does not have an RNI as the action of sunlight on the child’s skin will now be the major source of this vitamin. Parents and carers should give daily vitamin drops containing 10 micrograms of vitamin D to children aged 4 years or younger. For children aged 5 years and above, parents and carers can consider giving a daily supplement of 10 micrograms of vitamin D from October-March, when sunlight is not strong enough to make vitamin D in the skin.
7-10 years
There is a marked increase in requirements for energy and protein. There is no change in the requirement for thiamin, vitamin C or vitamin A. Children at this age have increased requirements for other vitamins and minerals.
11-14 years
Energy requirements continue to increase, and protein requirements increase by approximately 50%. By the age of 11 years, the vitamin and mineral requirements for boys and girls start to differ.
- Boys need more of all the vitamins and minerals.
- Girls need more of all the vitamins (except for thiamin, niacin, and vitamin B6) and minerals. Girls have a much higher iron requirement than boys (once menstruation starts).
15-18 years
Boys continue to have increased requirements for energy, protein, as well as several vitamins (thiamin, riboflavin, niacin, vitamins B6, B12, C and A) and minerals (magnesium, potassium, zinc, copper, selenium, and iodine). Calcium requirements remain high as skeletal development is rapid.
Girls have increased requirements for energy, protein, some vitamins (thiamin, niacin, vitamins B6, B12 and C) and minerals (phosphorus, magnesium, potassium, copper, selenium, and iodine). Girls have a higher requirement than boys for iron (due to menstrual losses) but a lower requirement for zinc and calcium
Boys and girls have the same requirement for vitamin B12, folate, vitamin C, magnesium, sodium, potassium, chloride, and copper.
Adults
19-50 years
In comparison to adolescents, energy requirements are lower for both men and women, as are requirements for calcium and phosphorus. There is also a reduced requirement in women for magnesium, and in men for iron. The requirements for protein and most of the vitamins and minerals remain virtually unchanged in comparison to adolescents (except for selenium in men which increases slightly). A daily supplement of 10 micrograms of vitamin D should be considered from October to March, when sunlight is not strong enough to make vitamin D in the skin. For more information on nutrition in adults, click here.
Pregnancy
During pregnancy, women have increased requirements for some, but not all, nutrients. The government's advice for women planning a pregnancy and in the first 12 weeks of pregnancy is to take a folic acid supplement to help reduce the risk of their child having a neural tube defect. Also, the advice for all women of childbearing age is to choose a diet that supplies adequate amounts of folate. Women who are pregnant only need extra energy and thiamin during the last 3 months of pregnancy. Mineral requirements do not increase. Women who are pregnant should consider taking a daily supplement of 10 micrograms of vitamin D from October to March when sunlight is not strong enough to make vitamin D in the skin.
Lactation
Women who are breastfeeding have an increased requirement for energy, protein, all the vitamins (except B6), calcium, phosphorus, magnesium, zinc, copper and selenium. Women who are breastfeeding should consider taking a daily supplement of 10 micrograms of vitamin D from October to March when sunlight is not strong enough to make vitamin D in the skin.
50+ years
Energy requirements decrease gradually after the age of 50 years in women and age 60 years in men as people typically become less active. Protein requirements decrease for men but continue to increase in women. The requirements for vitamins and minerals remain unchanged for both men and women. There is one exception - after menopause, women have a reduced requirement for iron to the same level as men. Adults aged 50 years and over should consider taking a daily supplement of 10 micrograms of vitamin D from October to March when sunlight is not strong enough to make vitamin D in the skin.
The reduction in energy needs, coupled with unchanged requirements for vitamins and minerals, means that the nutrient density of the diet becomes even more important. Nutrient density means the quantity of vitamins and minerals in relation to the amount of energy supplied by the foods and drinks consumed.