
As well as thinking about how what we eat affects our health, it’s also good to consider how it affects the planet. The good news is that healthier diets also tend to be more environmentally sustainable.
What is a healthy balanced diet?
The key to healthy eating is having a balance of different foods and nutrients in your diet.
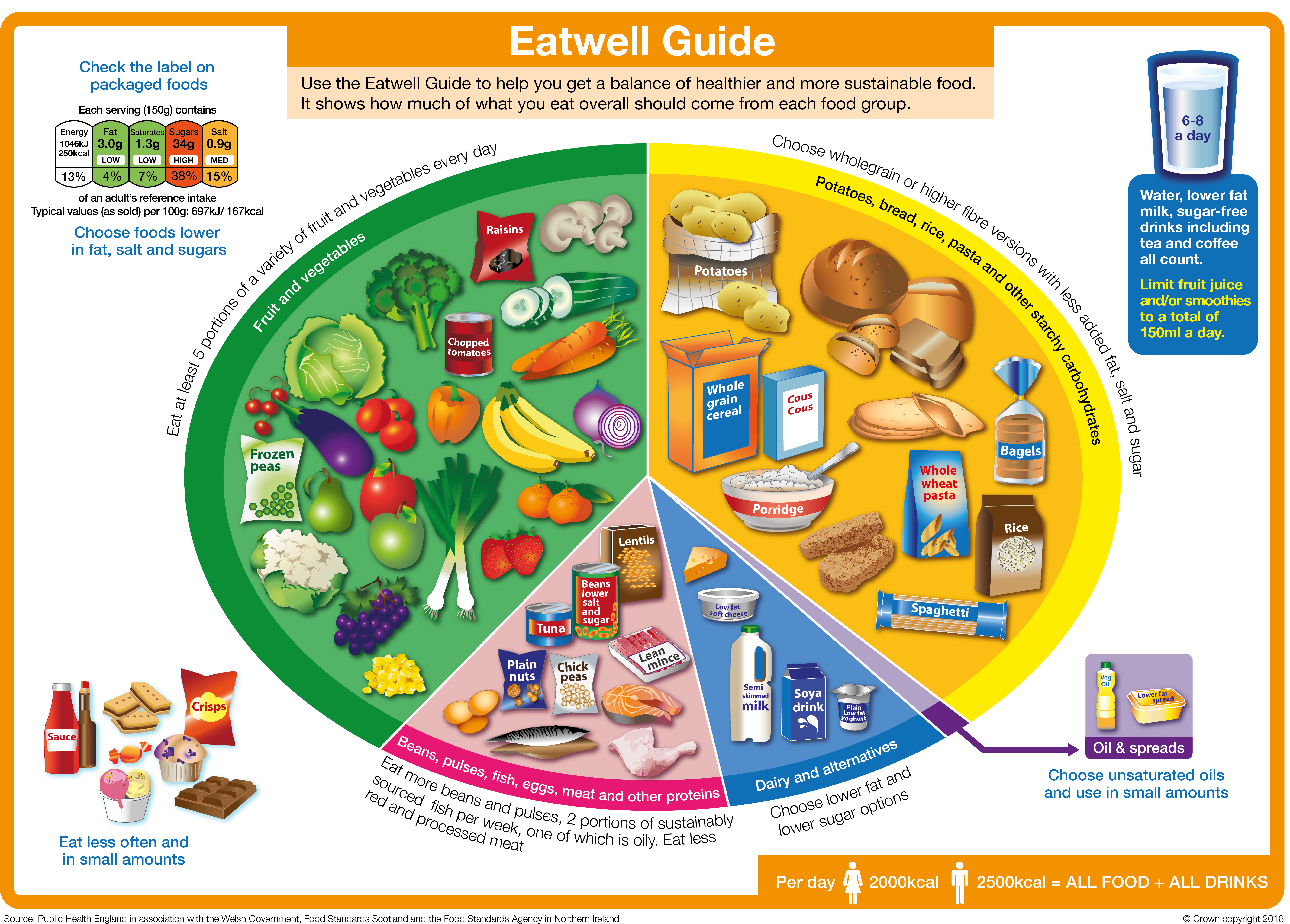
In the UK, the healthy eating model is called the Eatwell Guide.
There are a range of different types of eating (e.g. vegan and vegetarian) but the key principles of a healthy dietary pattern should run through all of these.
The six principles of healthy eating
Although there is no ‘one size fits all’ healthy diet, there are six principles we recommend.

At least 5 A DAY
Remember to include at least five portions of fruit and vegetables a day.

Fibre
Include plenty of fibre-rich foods, especially wholegrains.

Protein
Include a range of protein foods, especially beans, peas & lentils.

Dairy and alternatives
Include some dairy foods or fortified alternatives.

Choose the right fats
Mainly unsaturated fats and oils.

Limit
Eat fewer foods and drinks that are high in fat, salt and sugars.
Eating is not just about what we eat...
It's how too!
Mindful eating means being more aware of our thoughts, emotions and behaviours.
It is a non-judgemental approach that can help some people to develop a healthy relationship with food.
Join Dr Louise Durrant and Sarah Coe to explain how mindful eating may help some people to eat healthier, without the stigma or challenge of highly restrictive diets:

Key facts about healthy, balanced diets
- Fruit and vegetables are a key part of a healthy diet, and we should aim to get our 5 A DAY.
- Starchy foods like bread, potatoes, pasta, rice and other grains are part of a healthy diet, but the quality of what we choose is important.
- Plant-based protein foods, like beans and lentils, are naturally low in saturated fat and are sources of protein and fibre. We should aim to include these regularly in the diet.
- Animal protein foods like fish, eggs, meat and dairy provide a range of vitamins and minerals.
- Dairy foods provide protein, calcium, B vitamins and iodine.If choosing plant-based dairy alternatives, then look for those that are fortified with calcium and ideally other vitamins and minerals.

Why do I need a balanced diet?
Following a healthy, balanced diet helps make sure that our bodies get all the nutrients needed to work well and feel good. There’s plenty of evidence that shows eating healthily can also reduce the risk of diseases like heart disease, stroke, type 2 diabetes and some types of cancer.
Around the world, governments provide guidance on the balance of foods and drinks that make up a healthy diet. The guidelines vary in how they are presented but the message is similar; a healthy diet is about getting a balance and variety of foods from the main food groups.
What are the current healthy eating guidelines in the UK?
In the UK, our healthy eating model is called the Eatwell Guide. The guide has been developed scientifically, using modelling to look at the balance of different foods and drinks that provides the nutrients the body needs in the recommended amounts.
The Eatwell Guide shows the proportions that each of the food groups should make up in our diet and is designed to apply to most of us (although not to children under 2 years old as their dietary needs are different).
You can learn more about the Eatwell Guide on this page from the NHS.
The main food groups that feature in the Eatwell Guide, are outlined below. Each section has a useful guide to that food group.
Fruit and vegetables - eat more!
The fruit and vegetables group is the biggest in the Eatwell Guide and we are recommended to eat at least 5 A DAY. Diets high in fruit and vegetables are linked to a lower risk of diseases like heart disease, stroke and some types of cancer.
Fruit and vegetables provide a range of essential nutrients and fibre, as well as chemical compounds that occur naturally in plants that may have health benefits. Fruit and vegetables can also help you maintain a healthy weight as they are generally low in calories, so you can have plenty for relatively few calories.
Only 1 in 3 adults and 1 in 10 11-18 year olds are getting their 5 A DAY
Helena Gibson-Moore, Nutrition Scientist, British Nutrition Foundation
To get the most nutritional benefit out of your 5 A DAY it’s important to have a variety of fruits and vegetables. This is because different types and colours of fruits and vegetables contain different combinations of important nutrients such as:
- Vitamin C - important for keeping body tissues, such as skin and cartilage healthy.
- Vitamin A - important for normal vision, skin and the immune system.
- Folate - important for making red blood cells and supporting the immune system
- Potassium – important for healthy blood pressure and to support the nervous system
- Fibre – helps to maintain a healthy gut and can reduce the risk of diseases like type 2 diabetes and heart disease.
Did you know? Fresh, frozen, dried and canned fruits and vegetables all count towards our 5 A DAY.
Table 1: 5 A DAY. What counts as a portion?
|
Type |
What counts as a portion? |
|
Fresh, frozen or canned |
A portion of fruit or vegetables is 80g. This is around:
|
|
Dried and juice |
|
|
Beans and pulses
|
|
You can find out more about 5 A DAY portion sizes by reading this NHS page.
5 Top Tips For Eating More Fruit & Vegetables
- Add fresh or dried fruit to breakfast cereal or porridge
- Snack on fresh fruit or vegetable sticks
- Experiment with salads – you could try using red cabbage, adding brightly coloured vegetables such as grated carrot or sliced pepper and including leftover cooked vegetables like broccoli or peas in your salads.
- Add plenty of vegetables to dishes like pasta sauces, stews or curries – frozen or canned vegetables can be a quick and easy way to do this.
- Try fruit-based puddings like fruit salad or canned/dried fruits with plain yogurt
Starchy foods - go for wholegrain and higher fibre!
Also known as ‘carbs,’ starchy foods like bread, pasta, potatoes, rice and other grains are one of the main food groups included in healthy dietary guidelines all over the world.
These foods are sometimes (incorrectly) thought of as ‘fattening’ but what’s important is the types and portion sizes we eat
Sara Stanner, Science Director, British Nutrition Foundation
Starchy foods are a key source of fibre as well as vitamins and minerals such as iron, calcium, folate and B vitamins. For a healthier diet, we should choose more wholegrains and higher fibre starchy foods, such as wholemeal breads, wholemeal pasta, wholegrain breakfast cereals or oats and potatoes with skins.
Top tip! Try swapping white versions of bread, pasta or rice for wholegrain versions, go for wholegrains cereals or oats and try other types of wholegrains such as bulgur wheat, quinoa, freekeh, barley and spelt.
Looking for more information? Download: A guide to the food group 'Potatoes, bread, rice, pasta and other starchy carbohydrates'.
Protein foods - variety is key!
In the Eatwell Guide, this food group is called ‘Beans, pulses, fish, eggs, meat and other proteins'. This group of foods are a source of protein as well as other vitamins and minerals. It is a good idea to eat a variety of different types, and to include more plant-based sources of protein, such as beans, lentils or chickpeas, as these are higher in fibre and naturally low in fat.
Nuts and seeds (plain, unsalted) are included in this food group and contain vitamins, minerals and fibre. They are also high in fat but the majority of this is ‘healthier’ fat (unsaturated) and are a nutritious option in moderation (keeping portion sizes to just a small handful).
It’s recommended that we eat at least two portions (2 x 140g cooked weight) per week of sustainably sourced fish (fresh, frozen or canned), including a portion of oily fish. Oily fish includes salmon, sardines, mackerel and trout. Fish are sources of lots of vitamins and minerals. In particular, oily fish are natural sources of vitamin D and are the richest source of a special type of fat called long chain omega-3’s, which may help to prevent heart disease.
Meat can be part of a healthy diet and can be a source of several vitamins and minerals including iron, zinc and selenium. We are advised not to eat too much red or processed meat as high consumption has been linked with a higher risk of bowel cancer. You can cut down the fat content of meat by choosing leaner cuts such as lower fat mince, cutting off visible fat and taking the skin off poultry and using less fat when cooking, such as grilling instead of frying.
Looking for more information? Download: Beans, pulses, fish, eggs, meat and other proteins
Dairy foods and alternatives – go for lower sugar!
This food group includes milk, yogurt and cheese as well as plant-based alternatives to these. Dairy foods are an important source of calcium as well as protein, iodine and B vitamins. The nutritional content of dairy alternatives varies depending on what they are made from (such as soya, rice or oats) and whether they are fortified. If having dairy alternatives such as soya or oat milk, it’s best to choose those that are fortified with calcium and ideally other vitamins and minerals.
Dairy foods contain saturated fat, which we’re advised to eat less of (see below). Some studies suggest that despite their saturated fat content, dairy foods like milk, cheese and yogurt have a neutral effect on heart health. However, lower-fat versions of milk, cheese and plain yogurt are also lower in energy (calories) and so can be helpful if you are trying to manage your weight.
Fats and oils - choose unsaturated types!
There are different types of fats and oils in the diet – those that are mostly saturated such as butter, coconut oil, ghee, lard and palm oil, and those that are mostly unsaturated such as vegetable (usually rapeseed), sunflower and olive oils and spreads made from these. High intakes of saturated fat are linked to higher blood cholesterol and swapping saturated for unsaturated fats has been shown to reduce blood cholesterol and risk of heart disease. So it is a good idea to choose unsaturated fats and oils most of the time for cooking and spreading.
All fats are high in calories, even unsaturated fats, so it is important to use them in small amounts to avoid adding more calories than you need.
Looking for more information? Download: A guide to oils and spreads in the diet
Foods high in fat, salt and sugar – keep portions small!
Foods high in saturated fat, salt and sugar such as crisps, sweets, biscuits, cakes, chocolate and sugary drinks are not within the main food groups of the Eatwell Guide as they are not needed as part of a healthy diet. Sometimes called ‘treat foods’ we probably all know that these are foods to eat less of. If you do include them, then it is best to have small portions – for example, those that provide about 100-150kcal such as a small chocolate biscuit bar, 4 small squares of chocolate, 2 small biscuits, a small multipack bag of crisps, a mini muffin or a small chocolate mousse.
When it comes to sugary drinks it is best to swap these for water or sugar free versions.
What is the healthy eating guidance for different dietary patterns ?
The main food groups above are the building blocks of a healthy, balanced diet but they can be put together in different ways, based on our culture, preferences and dietary requirements. There are a whole range of different types of eating but the key principles of a healthy dietary pattern run through all of these
Applying these principles to your diet will help make sure it is balanced and healthy. There are a whole range of diets out there in books, in the press and on social media, some of which claim to have specific effects on health or to help with weight loss. It is not always easy to work out whether these diets are healthy – they may be promoted by doctors or mention scientific studies.
Diets that do not follow the healthy eating principles, for example those that cut out whole food groups, are probably going to be difficult to stick with and not likely to be good for your health in the longer term.
Zoe Hill, Nutrition Scientist, British Nutrition Foundation
The Mediterranean diet
The Mediterranean diet is often thought of as one of the healthiest eating patterns and features plenty of fruit, vegetables, pulses, wholegrains, olive oil, fish and smaller amounts of meat, dairy, eggs and sugary foods. A Mediterranean diet contains a higher proportion of fat than other healthy eating patterns, but most of this is unsaturated fats from olive oil, nuts and seeds and oily fish. This style of eating may reduce the risk of heart disease and have other potential health benefits. If this way of eating works for you then that’s great! However, it is not the only way to eat healthily, and may not work for everyone.
Vegetarian and vegan diets
Vegetarian and vegan diets have had a lot of interest and some research suggests that these diets may reduce the risk of heart disease. A healthy, balanced vegetarian or vegan diet will typically provide plenty of vegetables, pulses and wholegrains and so be rich in fibre and low in saturated fat.
Looking for more information? Read our page on vegetarian and vegan diets to find out more.
Plant-based diets
The term ‘plant-based diet’ is increasingly popular but there is some confusion about what it means. Some people think this refers to a vegetarian or vegan diet, but many authoritative bodies agree that plant-based eating means proportionately choosing more of your foods from plant sources and so is a diet mainly made up of plant foods, but may still include some meat, fish, eggs and dairy foods. Most healthy eating guidelines, including the Eatwell Guide recommend a mainly plant-based diet. The two biggest food groups; fruit and vegetables and starchy foods, are both plant-based and we are also encouraged to eat more beans and pulses and to use plant-based oils and spreads. So you can make your diet more ‘plant-based’ by including a wider variety of fruits and vegetables, including wholegrains as well as choosing more plant-based sources of protein.
Looking for more information? Read our information on how to put a healthy diet into practice including planners, tips and information on portion sizes.
At a glance:
- Research looking at the relationship between diet and health outcomes has shown a positive relationship between healthier dietary patterns and better health outcomes.
- To help people achieve a healthy balanced diet, governments around the world have developed food-based dietary guidance to illustrate what a healthy diet means in practice.
- Food-based dietary guidelines around the world vary in their presentation and format but the messages about the characteristics of healthy and balanced diets are relatively consistent.
- The UK Eatwell Guide was developed using optimisation modelling to find the proportions of the main food groups needed to fulfil current dietary recommendations.
- It has been estimated that following a dietary pattern consistent with the Eatwell Guide would benefit population health as well as being more environmentally sustainable.

What are dietary guidelines?
While nutrition recommendations often focus on individual nutrients or food components, food-based advice is important to help people put nutrition recommendations into practice.
Governments around the world have developed food-based dietary guidelines to communicate healthy eating recommendations in a nationally and culturally appropriate and practical way. The guidelines typically divide foods into food groups and provide advice on the proportion each of these groups should make up in the diet. Most guidelines also include a range of advice for people on how to put this into practice, including guidance on making healthier choices within the food groups (such as choosing wholegrain foods), how often to eat specific types of food (such as 5 A DAY), information on appropriate portion sizes as well tools such as planners or recipes.
While presentation of national food-based dietary guidance varies from country to country, the dietary pattern they present is broadly similar, with fruit and vegetables and starchy foods making up the largest groups, often with a particular focus on wholegrains. Dairy foods and protein food groups make up a smaller proportion, along with advice to limit foods high in fat, salt and sugar.
Redevelopment of UK food-based dietary guidance
UK food-based guidance has been through several iterations over the decades. Most recently, following changes to recommendations on fibre and free sugars in 2015, the government redeveloped the UK model the Eatwell Guide (then the Eatwell Plate) to take these changes into account.
Modelling was carried out by scientists at the University of Oxford using data on dietary intakes from the National Diet and Nutrition Survey (NDNS). Different scientific methods to recalculate the proportions of the food groups in the guide were considered and optimisation modelling using linear programming was selected. This used statistical techniques to model how current diets would need to change to meet current nutrition recommendations – both nutrient recommendations, such as those for fibre, and food-based recommendations, including 5 A DAY, were incorporated.
The results are summarised in Figure 1 below, showing that the proportion of foods from the fruit and vegetables and starchy foods groups would have to increase significantly and that the proportion of foods from all other groups would have to decrease. The food categories within the food groups did not always follow this pattern – in the ‘proteins’ food group, the modelling found that beans and pulses would have to increase by 90% and red meat would have to decrease by 78%.
Studies that have looked at the effect of following the Eatwell Guide compared to the average diet in the UK have found that it could significantly improve population health. One analysis carried out in 2016 when the Eatwell Guide was revised found that following the guidance (without increasing energy intake) could potentially avoid 17.8 million years of ill-health or early death (disability adjusted life years or DALYs) over the lifetime of the population.
Much of the benefit seen was due to prevention of type 2 diabetes as well as prevention of cancer and cardiovascular disease. Another analysis carried out in 2020, found that following at least five of the nine Eatwell Guide recommendations reduced mortality risk by approximately 7% as well as reducing carbon emissions by 30% compared to following 2 or fewer of the recommendations.
While there is increasing evidence for the benefits following healthier dietary patterns as set out in the Eatwell Guide and other models, we are a long way from making this a reality. As shown in the studies mentioned above, significant changes in eating habits are needed for current average UK diets to meet Eatwell Guide recommendations. It has been estimated that less than 1% of the population meet all current dietary guidelines and that only about 30% are meeting five or more of the nine specific recommendations in the Eatwell Guide.
Current UK diets are a long way from following the Eatwell Guide. Significant changes to diets are needed including increases in fruit and vegetable, fish and wholegrain consumption and reductions in foods high in saturated fat, salt and sugar
Anne de la Hunty, Senior Nutrition Scientist, British Nutrition Foundation
While trend data from the NDNS from 2008-2017 shows that there has been some progress in reducing intakes of free sugars and sugary drinks in recent years, intakes of free sugars, saturated fat and salt remain higher than recommended. There has been no appreciable increase in fruit and vegetable, fish, or fibre intakes. The broad principles of what makes up a healthy diet are well established but the challenge of how to encourage people in the population to take up this advice remains.
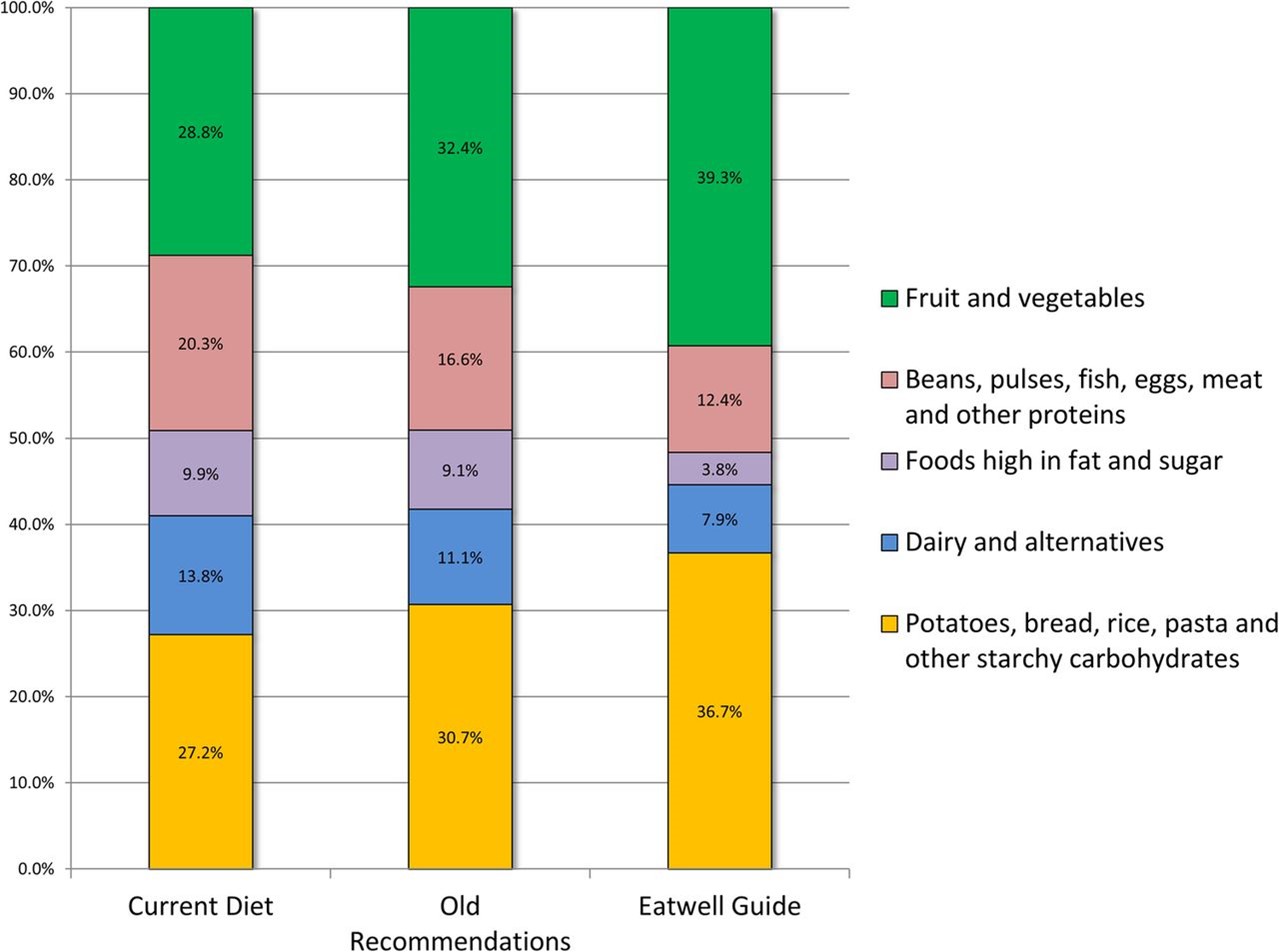
Breakdown of the diet by Eatwell Guide food group categories for current consumption, the ‘Eatwell Guide’ scenario and the ‘old recommendations’ (using previous recommendations for sugars and fibre) scenario
Scarborough et al. 2016
Research on dietary patterns
In recognition of the importance of dietary patterns rather than single foods or nutrients, researchers have developed methods for measuring healthy diets as part of cohort or intervention studies. This section will look at some examples of these measures and studies that have used them.
The Healthy Eating Index (HEI) is a measure of diet quality used to assess how well a set of foods aligns with key recommendations of the Dietary Guidelines for Americans.
The HEI-2015 includes 13 components that reflect the key recommendations in the 2015-2020 guidelines. There are two groups, ‘adequacy components’ and ‘moderation components’.
‘Adequacy components’ represent the elements of the diet that are encouraged in the guidelines. For these components, higher scores reflect higher intakes, because higher intakes are desirable.
The adequacy components are:
- Total fruit
- Whole fruit
- Total vegetables
- Greens and beans
- Wholegrains
- Dairy
- Total protein foods
- Seafood and plant proteins
‘Moderation components’ represent the foods or nutrients where there are recommended limits to consumption. In this case higher scores reflect lower intakes because lower intakes are more desirable.
The moderation components are:
- Refined grains
- Added sugars
- Saturated fats
- Sodium
Overall, a higher total HEI score suggests a diet that aligns better with the US dietary recommendations. Studies have found that greater adherence to the HEI is associated with lower risk of all-cause, cardiovascular and cancer mortality.
Alternative Healthy Eating Index (AHEI)
The AHEI was developed as an alternative to the HEI and focussed on foods and nutrients associated with reducing the risk of chronic disease. It is based on 11 components: six where the highest intakes are considered ideal (vegetables, fruit, whole grains, nuts and legumes, long chain omega-3 fats [docosahexaenoic acid and eicosapentaenoic acid], and polyunsaturated fatty acids), alcohol, for which moderate intake was considered ideal, and four components for which avoidance was recommended (sugar sweetened drinks and fruit juice, red and processed meat, trans fat and sodium). Each component is given a score between zero and ten, all the components adding up to a potential maximum score of 110, with higher scores suggesting better dietary quality.
The DASH diet
The DASH diet was developed to help lower blood pressure and it emphasises higher consumption of fruit, vegetables, legumes and nuts, wholegrains and low-fat dairy and limits sugary drinks, meat and sodium. The DASH score quantifies the level of adherence to the diet.
A systematic review and meta-analysis looking at dietary quality as assessed by the HEI, AHEI and the Dietary Approaches to Stop Hypertension (DASH) scores and health outcomes found that higher diet quality according to these methods was associated with reduced risk of all-cause mortality, reduced risk of cardiovascular and cancer incidence and mortality as well as reduced risk of type 2 diabetes and neurodegenerative disease.
The Nordic diet
The Nordic diet focuses on healthier foods that are locally produced in the Nordic region, and which are considered of importance to cultural and gastronomic identity in these countries. A Nordic style diet generally includes fruits such as apples, pears and berries, vegetables including roots, cruciferous vegetables and cabbages, as well as wholegrain and rye breads, a high intake of fish, low-fat dairy products, potatoes and vegetable fats.
Different scores have been developed to define a healthy Nordic diet, including the Baltic Sea Diet score (from Finland), Healthy Nordic Food Index (from Denmark) and the New Nordic Diet score (from Norway). Evidence from observational studies suggest that a Healthy Nordic is associated with lower risk of type 2 diabetes, stroke and a reduced risk of mortality (particularly from cardiovascular disease). Results from a small number of trials also suggest that a Nordic diet may help improve body weight, blood pressure and blood lipids. However, there is a general lack of evidence in non-Nordic populations to support these potentially beneficial effects if such a dietary pattern is adopted more widely.
Mediterranean diet
The Mediterranean diet, which is usually used to refer to the types of diets traditionally consumed in countries such as Italy and Greece, has been the subject of a lot of research over recent decades. Researchers have developed several different ways of measuring adherence to a Mediterranean dietary pattern. While these differ in exactly what is measured and how the score is calculated, higher consumption of fruit, vegetables, legumes, cereals, olive oil and fish and lower intakes of meat, dairy foods eggs and sugar are generally included. Research suggests that greater adherence to a Mediterranean diet may be associated with lower risk of coronary heart disease, lower levels of inflammation and a reduced risk of cognitive decline.
Plant-based diets
Plant-based diets have been the subject of much popular and scientific discussion in recent years. A set of plant-based diet indices have been developed as a research tool to investigate the health effects of such diets. The plant-based diet index (PDI) looks at the consumption of plant-based vs animal-based foods in the diet overall. The ‘healthful plant-based diet index’ (hPDI) emphasises plant-based foods that were considered to be healthy, including wholegrains, fruits, vegetables, nuts, legumes and tea and coffee. The ‘unhealthful plant-based diet index’ (uPDI) includes plant foods they considered as less healthy including fruit juices, refined grains, potatoes, sugary drinks and sweets. In each case, diets were scored according to their content of plant- vs animal-based foods and drinks, with an emphasis on healthy/less healthy plant-based elements for the hPDI and uPDI scores, respectively.
In a study looking at body weight in three large cohort studies, researchers found that a higher PDI score was associated with greater weight loss, but that this effect was greater with the hPDI score than the uPDI score. Another study looked at the association between these plant-based indices and risk of type 2 diabetes. The overall PDI score was associated with reduced risk although this was attenuated when it was controlled for body mass index (BMI). The hPDI score was associated with reduced risk of type 2 diabetes and the relationship remained after controlling for BMI. Conversely the uPDI score was associated with a higher risk of type 2 diabetes. A similar pattern was seen in a study looking at risk of coronary heart disease (CHD). The overall PDI score was associated with reduced risk of CHD, with a greater reduction seen with the hPDI score. Whereas the uPDI score was associated with increased risk of CHD.
Key references:
- EFSA (2010) Scientific Opinion on establishing Food-Based Dietary Guidelines https://www.efsa.europa.eu/en/efsajournal/pub/1460
- Morze et al. (2020) Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: A Second Update of a Systematic Review and Meta-Analysis of Cohort Studies. Journal of the Academy of Nutrition and Dietetics https://doi.org/10.1016/j.jand.2020.08.076
- PHE (2016) From Plate to Guide: What, why and how for the Eatwell model https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/579388/eatwell_model_guide_report.pdf
- Scarborough et al. (2016) Eatwell Guide: modelling the dietary and cost implications of incorporating new sugar and fibre guidelines. BMJ Open 6:e013182. http://dx.doi.org/10.1136/bmjopen-2016-013182
More on vitamins and minerals

A healthy balanced diet
We can probably all agree that eating a healthy, balanced diet is a good thing, but what does this mean in practice?
Healthy Diet FAQs
Is a healthy diet more sustainable?
Should I try a different diet if I am overweight?
There are a whole range of other popular diets such as keto, paleo or raw food diets, some of which claim to have specific effects on health or to help with weight loss. However, those diets which do not follow the healthy eating principles are typically harder to stick to and may be detrimental to your overall health in the longer term.
To lose weight, you need to create a calorie deficit in your diet. That means you need to burn more calories than you consume. To learn more about how to lose weight healthily read our page on healthy weight loss here.
Last reviewed October 2023. Next review due October 2026.